Which Shoulder of the Baby Gets Delivered First
Shoulder dystocia refers to a state of affairs where, afterward delivery of the head, the anterior shoulder of the fetus becomes impacted on the maternal pubic symphysis, or (less unremarkably) the posterior shoulder becomes impacted on the sacral promontory.
Information technology is an obstetric emergency, with an incidence of approximately 0.6-0.7% in all deliveries.
In this article, nosotros shall look at the hazard factors, clinical features and management of shoulder dystocia.
Pathophysiology
In normal labour, the fetal head is delivered via extension out of the pelvic outlet. This is followed by restitution of the fetal caput, and so it lies in a neutral position in relation to its spine. This means the fetal shoulders now prevarication in an anterior-posterior position.
Shoulder dystocia occurs when in that location is impaction of the anterior fetal shoulder behind the maternal pubic symphysis, or impaction of the posterior shoulder on the sacral promontory. A delay in delivery of the fetal shoulders leads to hypoxia in the fetus, proportional to the fourth dimension delay to complete commitment.
Applying traction on the fetal head can issue in fetal brachial plexus injury, and is major crusade for litigation in obstetrics.
[explanation id="attachment_13995" marshal="aligncenter" width="729"]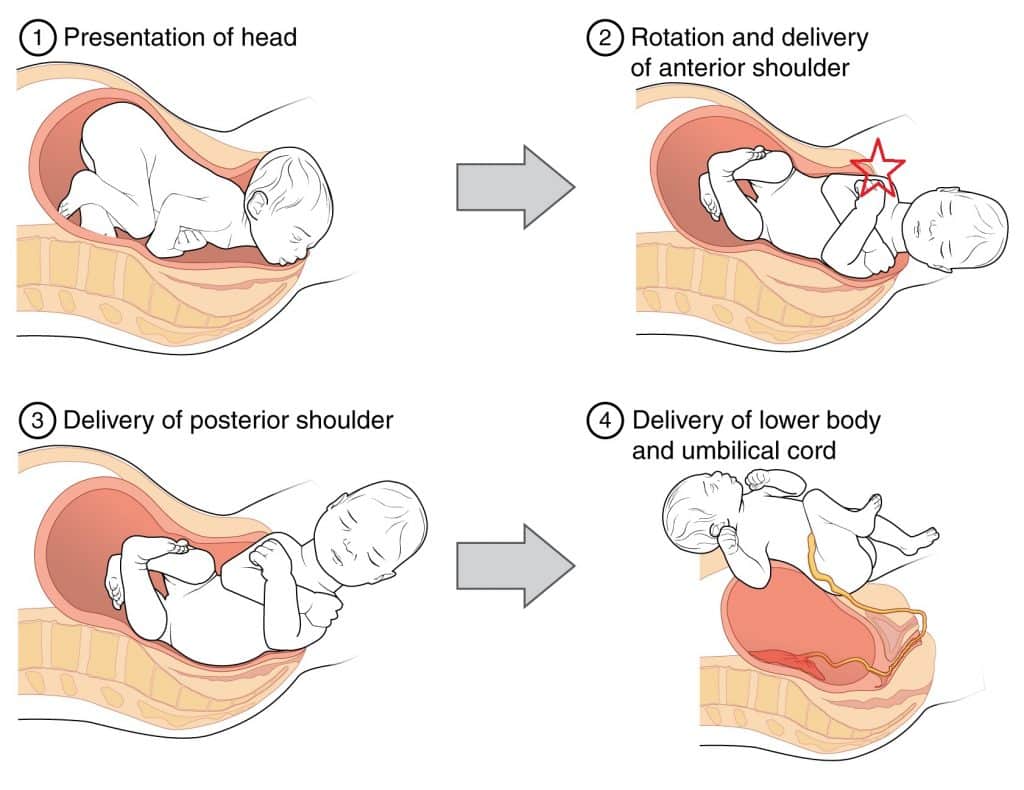 Fig one - The stages of normal childbirth. Shoulder dystocia unremarkably occurs at stage 2, where the anterior shoulder becomes impacted on the maternal pubic symphysis.[/caption]
Fig one - The stages of normal childbirth. Shoulder dystocia unremarkably occurs at stage 2, where the anterior shoulder becomes impacted on the maternal pubic symphysis.[/caption]
Risk Factors
The hazard factors for shoulder dystocia can exist divided into pre-labour and intrapartum factors:
| Pre-Labour | Intrapartum |
|
|
Clinical Features
Shoulder dystocia is defined past a delay in delivery of the shoulders post-obit the caput during a vaginal commitment with the next contraction later on using normal traction.
On examination, signs that may occur to help the diagnosis are:
- Difficulty in delivery of the fetal head or chin.
- Failure of restitution - the fetal remains in the occipital-anterior position after delivery by extension and therefore does not 'plough to look to the side'.
- 'Turtle Cervix' sign - the fetal caput retracts slightly back into the pelvis, and then that the neck is no longer visible, akin to a turtle retreated into its shell.
Management
Call back - If managed appropriately the risk of permanent brachial plexus injury can be well-nigh eliminated.
The immediate steps in the management of shoulder dystocia include:
- Phone call for help -shoulder dystocia is an obstetric emergency (volition need senior obstetrician, senior midwife and paediatrician in omnipresence).
- Advise the mother to finish pushing - this tin worsen the impaction.
- Avert downwards traction on the fetal head (increases risk of brachial plexus injury) – but utilize "routine" axial traction (i.east. keep the caput in line with the baby'due south spine), and exercise non apply fundal pressure (increases the run a risk of uterine rupture).
- Consider episiotomy - this will not relieve obstruction but can brand access for manoeuvres easier.
First Line Manoeuvres
- McRoberts manoeuvre - hyperflex maternal hips (knees to chest position) and tell the patient to stop pushing. This widens the pelvic outlet by flattening the sacral promontory and increasing the lumbosacral bending. This single manoeuvre has a success charge per unit of about ninety% and is even college when combined with 'suprapubic force per unit area', (encounter below).
- Suprapubic pressure is applied in either a sustained or rocking fashion to apply pressure behind the anterior shoulder to disimpact it from underneath the maternal symphysis.
[explanation id="attachment_13996" align="aligncenter" width="275"]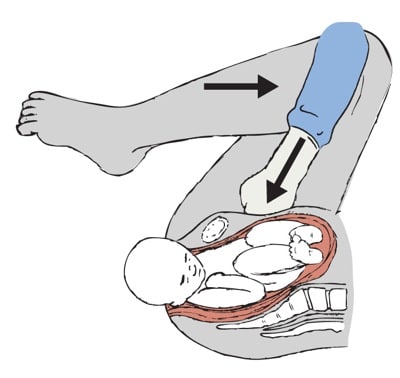 Fig 2 - The McRoberts manoeuvre - hyperflexion of the legs to increase the AP diameter of the pelvis.[/caption]
Fig 2 - The McRoberts manoeuvre - hyperflexion of the legs to increase the AP diameter of the pelvis.[/caption]
2d Line ('Internal') Manoeuvres
- Posterior arm – insert manus posteriorly into sacral hollow and grasp posterior arm to deliver.
- Internal rotation ("corkscrew manoeuvre") - apply force per unit area simultaneously in front of one shoulder and behind the other to motion baby 180 degrees or into an oblique position.
If the above manoeuvres fail then curlicue patient onto all foursand repeat (this may widen the pelvic outlet equally the legs are abducted and flexed).
Further Manoeuvers
These are only to exist considered when the above measures have been unsuccessful, and are very rarely used in the Britain:
- Cleidotomy - fracturing the fetal clavicle.
- Symphysiotomy - cut the pubic symphysis.
- Zavenelli - returning the fetal head to the pelvis for delivery of the baby via caesarean section.
Postal service-Delivery
After commitment of the fetus, active management of the third stage of labour is recommended (due to increased take chances of PPH). A PR examination should be performed to exclude a 3rd degree tear.
Shoulder dystocia tin can be a traumatic experience, particularly if the women does non have regional amazement. Debrief the mother and birth partner(south), and advise them of the risk of recurrence with any subsequent delivery.
Consider aphysiotherapist reviewbefore discharge, as women are at increased gamble of pelvic floor weakness/3rd degree tear, musculoskeletal hurting and temporary nervus impairment.
Additionally, apaediatric review is recommended before belch to appraise for brachial plexus injury, humeral fracture or hypoxic brain injury.
Complications
The complications of shoulder dystocia can be divided into maternal and fetal:
- Maternal - 3rd or 4th degree tears (3-4%), mail-partum haemorrhage (11%).
- Fetal - humerus or clavicle fracture, brachial plexus injury (two-16%), hypoxic brain injury.
[first-clinical]
Summary
- Shoulder dystocia is an obstetric emergency that tin lead to lasting injury to the baby.
- It is usually unpredictable, but there are chance factors that make information technology more probable, especially having had a previous baby with a shoulder dystocia and diabetes.
- Prompt management in a multi-disciplinary team volition lead to the all-time outcomes and grooming in skills drills is essential.
- The majority of shoulder dystocias are delivered past McRoberts manoeuvre.
[end-clinical]
Source: https://teachmeobgyn.com/labour/emergencies/shoulder-dystocia/
{kind=link}
Post a Comment for "Which Shoulder of the Baby Gets Delivered First"